Assessment of Vocal Fold Paralysis
Assessment of vocal fold paralysis typically consists of a few different measures performed by an otolaryngologist (ENT) and a Speech-Language Pathologist (SLP). The ENT and SLP must not only assess for vocal fold paralysis, but must also determine whether it is a unilateral or bilateral paralysis. As with all assessments, the assessment of vocal fold paralysis begins with the gathering of case history and background information. Instrumental and perceptual methods are then used to complete the assessment.
Instrumental Analysis
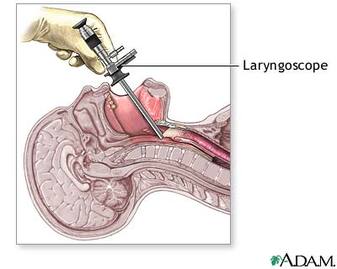
Example of a laryngoscope (drugline.com).
A procedure called a laryngoscopy is a common procedure that allows the ENT or SLP to visualize the vocal folds. There are two ways to perform a laryngoscopy. One way is the mirror laryngoscopy, during which a mirror is placed into the patient's mouth and a light is shined onto the mirror, allowing for visualization of the vocal folds with correct placement and angling of the mirror. This method is a quicker method that gives a quick overview of the status of the larynx. A second way is the endoscopic laryngoscopy, during which a light and a fiber optic scope is inserted into the patient, either orally or nasally, sending back images and/or recordings of the larynx. The rigid laryngoscope is inserted orally, and provides good lighting and magnification, but cannot assess the entire vocal tract and can only assess sustained vowels. The flexible laryngoscope is inserted nasally; it can assess the entire vocal tract and connected speech, but has poorer magnification than the rigid laryngoscope. Videostroboscopy is an endoscopic procedure that allows for a slow motion, frame-by-frame, analysis of the vocal folds. This is useful for viewing the vibration of the vocal folds in action.
During the laryngoscopy, the SLP and ENT carefully observe the vocal fold behavior for signs of paralysis. In a bilateral paralysis, both of the vocal folds would be observed to be fixed in either an abducted or adducted position. Both of these conditions are life threatening, as a permanently adducted state would hinder breathing and a permanently abducted state would put the patient at risk for aspiration while swallowing. In a unilateral paralysis, the ENT or SLP would observe that the paralyzed vocal fold remains in an abducted position while the functioning fold moves towards the midline during phonation, creating an open space in the vocal folds when they should be closed.
During the laryngoscopy, the SLP and ENT carefully observe the vocal fold behavior for signs of paralysis. In a bilateral paralysis, both of the vocal folds would be observed to be fixed in either an abducted or adducted position. Both of these conditions are life threatening, as a permanently adducted state would hinder breathing and a permanently abducted state would put the patient at risk for aspiration while swallowing. In a unilateral paralysis, the ENT or SLP would observe that the paralyzed vocal fold remains in an abducted position while the functioning fold moves towards the midline during phonation, creating an open space in the vocal folds when they should be closed.
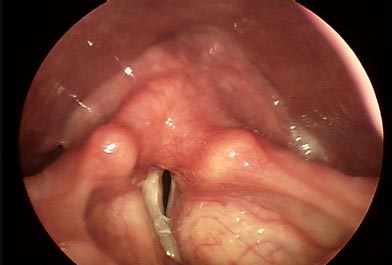
Image of unilateral vocal fold paralysis. (NYEE, 2013).
Example of a laryngeal electromyography.
(Heman-Ackah & Barr, 2006).
Another important measure that can be used to assess for vocal fold paralysis is laryngeal electromyography, or LEMG. An LEMG requires placing small electrodes on the muscles surrounding the vocal folds. The patient is asked to perform a series of vocal tasks, during which time the electrical responses from the muscles are recorded. Analysis of the pattern of the electrical waves yields information as to: whether the vocal cords are paralyzed, the site of lesion, and the severity of nerve damage. The LEGM can be very useful in differentiating vocal cord paralysis from other disorders, such as cricoarytenoid joint fixation, and can also provide prognostic information regarding the likelihood of regaining phonation without surgery.
As vocal fold paralysis may be caused by a number of diseases, other tests may be needed to include or exclude the cause of nerve injury to the vocal folds. Additional tests may include blood tests, lung function tests, X-rays, MRIs, and CT scans.
As vocal fold paralysis may be caused by a number of diseases, other tests may be needed to include or exclude the cause of nerve injury to the vocal folds. Additional tests may include blood tests, lung function tests, X-rays, MRIs, and CT scans.

Acoustic analysis in progress. (University of the Pacific, 2013).
Acoustic analysis of the voice is another instrumental measure that can be used to assess for vocal fold paralysis. Using computer software such as Visi-Pitch IV, The Computerized Speech Software Lab, and the Nagashima Phonatory Function Analyzer, the SLP is able to visualize different parameters of the voice. The patient is prompted to speak into a microphone attached to the computer, and the patient's vocalizations are recorded and then produced into waveforms which the SLP analyzes. The SLP looks at different aspects of the waveform which correlate to the pitch, loudness, fundamental frequency, jitter (fluctuation in pitch), and shimmer (fluctuation in loudness) of the voice to determine if the patients vocal qualities are within normal limits for their gender and age.
A patient with vocal fold paralysis will produce speech that creates a different waveform than that of normal speakers. In research conducted by Patal and Parsram in 2005, it was found that individuals with unilateral vocal fold paralysis exhibited more fluctuation per second in fundamental frequency, fluctuation per second in amplitude, extent of fluctuation in fundamental frequency, extent of fluctuation in amplitude, jitter ratio, jitter factor, and shimmer than subjects without vocal fold paralysis. Their research also suggests that acoustic analysis alone can lend information as to whether the patient suffers from right vocal fold paralysis of left vocal fold paralysis.
A patient with vocal fold paralysis will produce speech that creates a different waveform than that of normal speakers. In research conducted by Patal and Parsram in 2005, it was found that individuals with unilateral vocal fold paralysis exhibited more fluctuation per second in fundamental frequency, fluctuation per second in amplitude, extent of fluctuation in fundamental frequency, extent of fluctuation in amplitude, jitter ratio, jitter factor, and shimmer than subjects without vocal fold paralysis. Their research also suggests that acoustic analysis alone can lend information as to whether the patient suffers from right vocal fold paralysis of left vocal fold paralysis.
Perceptual Analysis
SLPs are not forced to rely purely on instrumental methods to make their assessments. SLPs further incorporate their clinical knowledge and experience into the assessment process by performing perceptual analyses of the patient's voice. During this procedure, the SLP has the patient perform a range of vocal tasks which may include sustained phonation, reading, and spontaneous conversation. The SLP listens to different parameters of the voice such as pitch, loudness, and quality to determine if the voice sounds normal and healthy. The SLP may conduct these analyses in the office or may chose to observe the patient out of the office in their everyday speaking environments. The SLP may also ask the patient questions about how their voice impacts their overall quality of life and communicative experiences to get a better idea of how the patient is being impacted by their vocal problems.
A patient with unilateral vocal fold paralysis will exhibit dysphonia or aphonia. Some perceptual characteristics that are associated with unilateral vocal fold paralysis include a breathy and/or hoarse vocal quality, reduced phonation time, decreased loudness, inability to change loudness, diplophonia, and pitch breaks. The breathy quality, reduced loudness, and shorter phonation time are due to the escape of air through vocal folds that are not completely adducted during phonation. The hoarse vocal quality, pitch breaks, and diplophonia can be caused by the inability to adjust the tension of the paralyzed vocal fold. Additional tension above the glottis may also add to the hoarse vocal quality.
A patient with unilateral vocal fold paralysis will exhibit dysphonia or aphonia. Some perceptual characteristics that are associated with unilateral vocal fold paralysis include a breathy and/or hoarse vocal quality, reduced phonation time, decreased loudness, inability to change loudness, diplophonia, and pitch breaks. The breathy quality, reduced loudness, and shorter phonation time are due to the escape of air through vocal folds that are not completely adducted during phonation. The hoarse vocal quality, pitch breaks, and diplophonia can be caused by the inability to adjust the tension of the paralyzed vocal fold. Additional tension above the glottis may also add to the hoarse vocal quality.
A combination of these instrumental and perceptual assessment tools will allow the ENT and SLP to determine the presence and severity of vocal fold paralysis. If vocal fold paralysis exists, the SLP and ENT work together to create an appropriate and individualized treatment plan for the patient.
